

The woodland has a number of blogs in relation to ‘therapy resistant despair’ taking a look at a spread of subjects from the affected person expertise to the associated fee effectiveness of interventions similar to long run psychoanalytic psychotherapy.
I put therapy resistant despair (TRD) in italics above as it’s possible you’ll be shocked to know that there isn’t a consensus on its definition, which in flip implies that the incidence charges fluctuate and there are not any constant scientific tips in relation to therapy (Gabriel et al 2023).
The US Meals and Drug Administration and the European Medicines Company have adopted probably the most used definition of TRD (insufficient response to a minimal of two antidepressants regardless of adequacy of the therapy trial and adherence to therapy). It’s presently estimated that at the least 30% of individuals with despair meet this definition and so the burden of this side of despair shouldn’t be insignificant (McIntyre R et al 2023).
The Maudsley Prescribing Pointers (Taylor et al 2021) first selection choices for administration of TRD embrace augmentation with lithium and quetiapine. This weblog seems on the new randomised managed trial by Prof Tony Cleare et al, printed at present in The Lancet Psychiatry, straight evaluating the scientific and value effectiveness of the 2. This paper is especially attention-grabbing because the trial (the LQD examine (Lithium versus Quetiapine in Melancholy)) has a for much longer comply with up interval than earlier research, enabling a ‘actual life’ comparability.
The LQD examine, printed at present within the Lancet Psychiatry compares the scientific and value effectiveness of lithium and quetiapine for therapy resistant despair.
Strategies
So, this trial is a *takes a deep breath* “section 4, pragmatic, open label, parallel-group, randomised managed superiority trial, evaluating the scientific effectiveness and value effectiveness of lithium versus quetiapine augmentation of antidepressant remedy in individuals with treatment-resistant despair.”. Let me break that down for you:
- Section 4: remedy is authorised and being utilized in apply. These trials have a look at long run security and effectiveness in apply
- Pragmatic: trying on the effectiveness of medicines in actual life conditions
- Open label: individuals and researchers know which therapy the individuals are receiving (non-blinded examine)
- Parallel group: two energetic therapy teams, that are then in contrast
- Randomised managed superiority trial: individuals had been randomly assigned to therapy teams and reviewed as to which therapy performs higher.
Scientific effectiveness course of: Following random allocation to therapy, trial clinicians might determine whether or not to proceed with prescription of the allotted remedy based mostly on pre-prescribing security checks and scientific judgement. All individuals, no matter trial remedy standing, had been adopted up over 12 months until they actively withdrew.
The first outcomes had been:
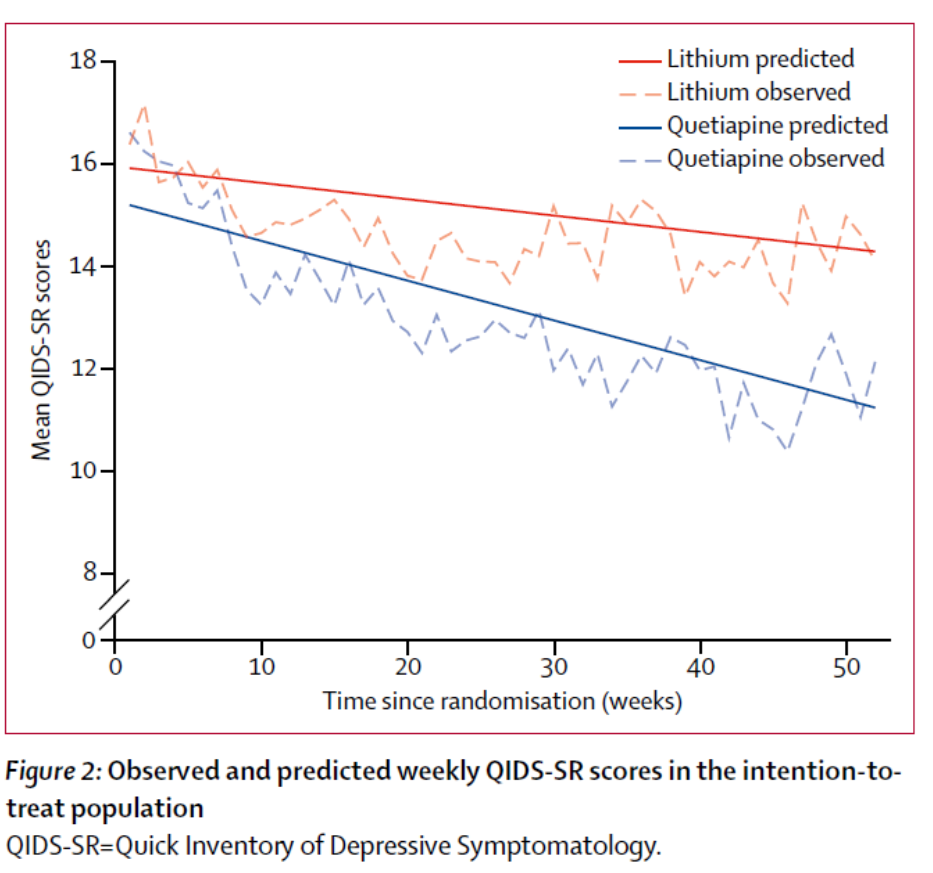
- The Fast Stock of Depressive Symptomatology (QIDS-SR) , used as a weekly measure of temper state and
- Time to discontinuation of therapy.
Weekly information on QIDS-SR, Work and Social Adjustment Scale (WSAS) and trial remedy standing had been collected through a web based platform, True Colors.
Value effectiveness course of: The Consumer Service Receipt Stock was used at baseline, 8, 26, and 52 weeks. This software collects information on health-care service use, together with the quantity and length of contacts with major and secondary health-care companies. High quality-Adjusted Life Years (QALYs) had been used to measure well being advantages.
Outcomes
Over a 4.5 yr interval (Dec 2016 to July 2021) 262 sufferers had been screened for eligibility from 6 NHS Trusts throughout England. The inclusion standards included:
- ≥ 18 years
- Below the care of a GP or psychological well being service
- Present depressive episode assembly DSM-5 standards for main depressive dysfunction (single or recurrent episode)
- Rating of ≥ 14 on the 17 merchandise Hamilton Melancholy Score Scale
- Insufficient response of the present episode to 2 or extra antidepressants, prescribed for at the least 6 weeks at therapeutic dose
- Present antidepressant therapy unchanged and at therapeutic dose for at the least 6 weeks; and
- Had been capable of present written knowledgeable consent
Exclusion standards included (however not restricted to)
- Prognosis of bipolar dysfunction or present psychosis
- Enough use of lithium or quetiapine of their present episode
- Present use of one other atypical antipsychotic.
There have been major, secondary and tertiary outcomes within the examine. For this weblog I’ll give attention to the first outcomes and notice any key outcomes from the secondary outcomes (tertiary outcomes weren’t included on this publication).
212 sufferers had been randomly assigned:
- 105 assigned to lithium; 21 didn’t obtain or provoke lithium however remained within the trial. 66 supplied information at 52 week comply with up
- 107 assigned to quetiapine; 12 didn’t obtain quetiapine however remained within the trial. 78 supplied information at 52 week comply with up
Scientific effectiveness outcomes
Major outcomes
- General burden of depressive symptom severity over 12 months
- Time to all trigger discontinuation
Contributors within the quetiapine group had a decrease general burden of depressive symptom severity than individuals within the lithium group over 12 months. The QIDS-SR information factors had been mapped over the yr and the realm underneath the curve calculation used as a measure of depressive symptom burden. The world underneath the curve was smaller for Quetiapine: (space underneath the distinction curve –68.36 [95% CI –129.95 to –6.76]; p=0.0296).
Time to trial remedy discontinuation didn’t differ considerably between the 2 teams; the median time was:
- 365.0 days (Inter-Quartile Vary, IQR 57.0 to 365.0) within the quetiapine group
- 212.0 days (21.0 to 365.0) within the lithium group
- Adjusted hazard ratio [HR] 0.72 [95% CI 0.47 to 1.09]; p=0.1196.
Given the broad IQR and huge discrepancy between the respective medians, we should think about this “absence of proof” somewhat than “proof of absence”.
By way of secondary outcomes, individuals within the quetiapine group had considerably decrease MADRS (p=0.0435) and WSAS scores (p=0.0071) at week 52 than individuals within the lithium group. No important variations had been famous within the different secondary outcomes which included bodily well being parameters and opposed occasions (see paper for full particulars). An attention-grabbing adverse consequence was that no weight achieve was noticed throughout time within the quetiapine group.
Value effectiveness outcomes
In contrast with lithium, quetiapine was dominant. Prices had been decrease whereas advantages had been greater.
From an NHS and private social companies perspective, quetiapine was related to decrease price and bigger achieve in QALYs, than lithium. The incremental web well being good thing about Quetiapine was 0.097 over lithium (with any constructive consequence indicating desire to the in contrast various). Further price effectiveness evaluation can be found within the appendices of the paper which define that quetiapine is probably the most cost-effective choice in accordance with the NICE willingness-to-pay threshold.
The quetiapine therapy group had a decrease general burden of depressive symptomatology than lithium.
Conclusions
The authors concluded that:
our findings recommend a average and clinically related good thing about quetiapine over lithium for long-term therapy of individuals with treatment-resistant despair.
And this examine:
…extends the earlier discovering that quetiapine is non-inferior to lithium over the quick time period and recommend superiority over the long term.

In comparison with lithium, quetiapine is probably the most cost-effective choice in relation to the NICE willingness-to-pay threshold.
Strengths and limitations
This paper has some actual strengths in that its major goal was to imitate real-life scientific selections and sufferers. There was lived expertise involvement in designing and operating the trial and affected person and public involvement members had been supportive of the weekly QIDS-SR assessments to supply a greater indication of the course and long-term length of final result for what could be a fluctuating scientific course in therapy resistant despair (TRD). Following sufferers up for 1 yr was a giant plus.
Because of the nature of the trial, clinicians weren’t blind to allocation, nevertheless the authors report that ‘clinician rated final result measures had been assessed by masked raters and statisticians had been unaware of group allocation till the information evaluation section’ to try to cut back bias as a lot as doable.
With each trial there will probably be limitations and this paper isn’t any exception. Having clinician judgement as as to if the allotted medication is prescribed doubtlessly introduces allocation bias.
The affected person teams had been randomised in accordance with diploma of therapy resistance (failure of two versus three or extra antidepressant therapies within the present episode) and so they used ‘block randomisation with randomly various block sizes’, nevertheless inside the outcomes there isn’t a reference as to what number of had been in every group or whether or not the outcomes correlated to this.
A lot of the information relied on self-reports. Though this methodology was developed in partnership with affected person teams, the burden could have contributed to attrition.
In the course of the trial, the pattern measurement was decreased from 276 to 214 as a result of challenges with recruitment. Energy calculations had been accomplished and had been 80% for time to discontinuation and 96.5% energy with an impact measurement of 0.38. It’s nevertheless unclear if the discontinuation charges, impact sizes and attrition charges had been modified from the unique planning when calculating these. There gave the impression to be doubtlessly regarding gaps within the 52 week assortment information, extra so for lithium (37% for the lithium group and 27% for the Quetiapine group) and the authors notice substantial lacking information for among the secondary outcomes.
General, there was plenty of attrition, which ought to warning our interpretation of those outcomes. The intention to deal with evaluation solely included 66/104 and 78/107 of the lithium and quetiapine sufferers respectively. The totally different ranges of attrition in every group could imply that we’re now not evaluating like with like throughout the teams.
Lastly, the inhabitants examined was predominantly white (89%) which can restrict the flexibility for generalisation to all populations.

Mimicking actual life scientific apply over a yr comes with it’s personal limitations.
Implications for apply
Sufferers who’ve despair which is ‘tough to deal with’ are ‘clinically difficult’ and undergo a big burden from the illness. Each lithium and quetiapine are widespread choices for augmentation and this paper highlights that quetiapine may very well be extra efficacious and value efficient than lithium. The size of comply with up of the examine makes this encouraging and positively price contemplating. The ability of the examine and the somewhat heterogeneous group of severity could restrict leaping to a direct use of quetiapine over lithium, but when there was future replication of this examine and outcomes, then that will surely be convincing.
The authors are clear although that Lithium stays an efficient therapy choice. It’s probably that the drugs could have totally different advantages for various individuals (e.g. considerations in relation to sleep, urge for food, nervousness) and so therapy ought to be tailor-made to those wants. Nonetheless, if lithium and quetiapine are equally acceptable then quetiapine may pip lithium to the submit.
Having clear scientific tips in relation to methods for ‘tough to deal with’ despair and/or when it turns into ‘therapy resistant’, appears a precedence in order that future analysis could be evaluating apples with apples.
On the time of penning this, there’s a complicating consider that there’s a nationwide scarcity of modified launch quetiapine and we’re having to maneuver sufferers onto rapid launch Quetiapine which has a special aspect impact profile and should not produce outcomes replicable to the examine.
Quetiapine could pip lithium to the submit if on a good area.
The private affect of therapy resistant despair can’t be underestimated and I’m certain they’d agree with the phrases of Bon Jovi ‘I simply need to reside whereas I’m alive…it’s my life’.
Assertion of pursuits
I’ve no battle of pursuits to reveal
Hyperlinks
Major paper
Anthony J Cleare, Jess Kerr-Gaffney, Kimberley Goldsmith, Zohra Zenasni, Nahel Yaziji, Huajie Jin, Alessandro Colasanti, John R Geddes, David Kessler, R Hamish McAllister-Williams, Allan H Younger, Alvaro Barrera, Lindsey Marwood, Rachael W Taylor, Helena Tee, and on behalf of he LQD Research Group. (2025) Scientific and cost-effectiveness of lithium versus quetiapine augmentation for treatment-resistant despair in England: a realistic, open-label, parallel-group, randomised managed superiority trial. The Lancet Psychiatry 2025. DOI: 10.1016/S2215-0366(25)00028-8
Different references
Gabriel FC et al (2023) Pointers’ suggestions for the treatment-resistant despair: A scientific overview of their high quality. PLoS ONE 18(2): e0281501.
McIntyre RS, et al (2023) Therapy-resistant despair: definition, prevalence, detection, administration, and investigational interventions. World Psychiatry. (2023) 22, no. 3, 394–412.
Taylor, David M, et al. The Maudsley Prescribing Pointers in Psychiatry. 14th ed., John Wiley & Sons, 2021 pg 318-319.



